인간 성 해부학과 생리학(Human Sexual Anatomy and Physiology)
인간 성 해부학과 생리학
By Don Lucas and Jennifer FoxNorthwest Vista College
해부학과 생리학에 대해 호기심을 갖는 것은 당연한 일입니다. 해부학과 생리학에 대한 지식은 즐거움, 신체적, 정신적 건강, 삶의 만족도를 높일 수 있는 잠재력을 높여줍니다. 개인적인 호기심을 넘어 성 파트너와 해부학 및 생리학에 대해 사려 깊은 대화를 나누면 잘못된 의사소통, 의도하지 않은 임신, 성병 감염, 성기능 장애의 가능성을 줄일 수 있습니다. 마지막으로, 가장 중요한 것은 성적 호기심, 욕망, 뇌의 능력 뒤에 있는 생물학적, 심리적 동기를 모두 이해하는 것이 관계의 건강을 증진할 수 있다는 것입니다.
Learning Objectives
- Explain why people are curious about their own sexual anatomies and physiologies.
- List the sexual organs of the female and male.
- Describe the sexual response cycle.
- Distinguish between pleasure and reproduction as motives behind sexuality.
- Compare the central nervous system motivating sexual behaviors to the autonomic nervous system motivating sexual behaviors.
- Discuss the relationship between pregnancy and birth control.
- Analyze how sexually transmitted infections are associated with sexual behaviors.
- Understand the effects of sexual dysfunctions and their treatments on sexual behaviors.
- 사람들이 자신의 성 해부학과 생리에 대해 궁금해하는 이유를 설명하세요.
여성과 남성의 성기를 나열합니다.
성적 반응 주기를 설명하십시오.
성행위의 동기로 쾌락과 생식을 구별합니다.
성적 행동에 동기를 부여하는 중추 신경계와 성적 행동에 동기를 부여하는 자율 신경계를 비교하십시오.
임신과 피임의 관계에 대해 토론하십시오.
성병이 성행위와 어떻게 연관되어 있는지 분석합니다.
성기능 장애와 그 치료가 성 행동에 미치는 영향을 이해합니다.
Introduction
대부분의 사람들은 섹스에 대해 궁금해합니다. Google은 하루에 35억 건 이상의 검색 쿼리를 처리하며(Google 검색 통계)이 중 수천만 건은 익명으로 처리되는 성에 관한 검색입니다. Google에서 섹스와 관련하여 가장 자주 묻는 질문은 무엇인가요? 혼외정사에 관한 질문인가요? 변태적인 환상에 관한 질문인가요? 성적인 체위? 놀랍게도, 아닙니다. "내 성기는 얼마나 커야 하나요?", "질에서 식초 냄새가 나는 것이 건강에 좋은가요?" 등 실용적이고 단순한 질문이 많으며, 성 해부학에 관한 질문이 대부분입니다(Stephens-Davidowitz, 2015). 또한 Google은 사람들이 다른 사람의 해부학적 구조보다 자신의 성기 해부학적 구조에 훨씬 더 관심이 많으며, 예를 들어 남성이 여성보다 성기에 대해 질문할 확률이 170배 더 높다는 사실을 밝혀냈습니다(Stephens-Davidowitz, 2015). Google에서 성에 관해 두 번째로 자주 묻는 질문은 "남자친구를 더 빨리 절정에 이르게 하려면 어떻게 해야 하나요?"와 같은 성 생리에 관한 질문입니다. "섹스는 왜 고통스러운가요?", "오르가즘이란 정확히 무엇인가요?"와 같은 질문입니다. 이러한 검색은 사람들이 성 해부학과 생리학에 대한 매우 기본적인 질문에 큰 관심을 가지고 있다는 것을 보여줍니다.

그러나 성에 관한 질문에 대해 친구, 가족, 심지어 인터넷 '권위자'로부터 얻는 답변의 정확성은 신뢰할 수 없는 경우가 많습니다(Fuxman et al., 2015; Simon & Daneback, 2013). 예를 들어, Buhi와 동료들(2010)이 177개의 성 건강 관련 웹사이트의 콘텐츠를 조사한 결과, 거의 절반에 부정확한 정보가 포함되어 있는 것으로 나타났습니다. 이 모듈의 저자인 저희는 여러분께 약속을 드리는 것은 어떨까요? 이 모듈에는 성 해부학 및 생리학에 대해 궁금해하는 많은 질문에 대한 편견 없는 과학적 근거를 바탕으로 한 답변이 포함되어 있으므로, 이 자료를 배우신다면 더 이상 비밀리에 구글을 찾아다닐 필요가 없을 것입니다.
'성적으로 노골적인 언어'에 대한 새로운 시각을 접할 준비가 되셨나요? 이 모듈은 성이라는 흥미로운 주제를 다루고 있지만, 여러분에게 새롭거나 혼란스러울 수 있는 어휘가 포함되어 있습니다. 이 어휘를 배우려면 추가적인 노력이 필요할 수 있지만, 이러한 용어를 이해하면 성관계와 자신을 더 잘 이해할 수 있을 것입니다.
마스터스와 존슨
사람들은 항상 섹스를 해왔지만 이에 대한 과학적 연구는 비교적 최근까지 금기시되어 왔습니다. 사실 성 해부학, 생리학, 행동에 대한 연구는 19세기 후반에야 공식적으로 시작되었고, 1950년대에 들어서야 진지하게 받아들여지기 시작했습니다. 특히 1957년 윌리엄 마스터스(1915~2001)와 버지니아 존슨(1925~2013)은 연구팀을 구성하여 사람들에게 단순히 성생활에 대해 묻는 것에서 실제로 성관계를 갖는 동안 사람들의 해부학과 생리를 측정하는 것으로 성에 대한 연구를 확장했습니다. 마스터스는 전직 해군 중위이자 두 아이의 아버지였으며 매춘부 연구에 관심이 있는 산부인과 전문의였습니다. 존슨은 전직 컨트리 음악 가수이자 두 아이의 미혼모, 세 번의 이혼, 두 번의 대학 중퇴를 경험했으며 사회학 공부에 관심이 있었습니다. 궁금하신 분들을 위해 말씀드리자면, 마스터스와 존슨은 (마스터스가 아직 결혼하지 않았을 때) 연인이었고, 결국 결혼했지만 나중에 이혼했습니다. 화려한 사생활에도 불구하고 두 사람은 과학적 관점에서 성을 이해하는 데 관심을 가진 헌신적인 연구자였습니다.
마스터스와 존슨은 주로 맥박과 혈압 측정뿐만 아니라 유방, 피부, 다양한 근육 구조, 방광, 직장, 외부 성기, 폐 등 다양한 신체 부위의 성적 반응을 파악하기 위해 혈류측정법(장기로 가는 혈액 또는 공기 흐름의 변화를 측정하는 방법)을 사용했습니다. 연구팀은 700명(18~89세)을 대상으로 파트너와의 성관계 또는 혼자서 성관계를 갖는 동안 10,000회 이상의 오르가즘을 측정했습니다. 마스터스와 존슨의 연구 결과는 처음에 두 권의 베스트셀러 책으로 출판되었습니다: 인간의 성적 반응, 1966년과 인간의 성적 부적응, 1970년. 이들의 초기 실험 기법과 데이터는 성 해부학과 생리학에 대한 현대적 이해의 토대를 형성했습니다.
쾌락과 생식의 해부학
성 해부학은 일반적으로 생식의 관점에서만 논의됩니다(예: King, 2015 참조). 그러나 생식은 우리를 성적으로 움직이는 원동력의 (작은) 일부일 뿐입니다(Lucas & Fox, 2018). 성 해부학에 대한 완전한 논의에는 쾌락의 개념도 포함됩니다. 따라서 여기서는 생식과 쾌락에 대한 능력 측면에서 여성(그림 1a 및 1b 참조)과 남성(그림 2 참조)의 성적 해부학을 살펴볼 것입니다.

여성 해부학
많은 사람이 여성의 성 해부학에 대해 호기심과 혼란스러움, 신비함을 느낍니다. 이는 많은 부분이 신체 내부에 있기 때문일 수도 있고, 역사적으로 여성은 자신의 신체에 대해 겸손하고 비밀스러워야 한다고 여겨져 왔기 때문일 수도 있습니다.
여성의 성 해부학에서 가장 눈에 잘 띄는 구조는 아마도 외음부일 것입니다. 외음부의 주요 기능은 쾌락과 보호입니다. 외음부는 여성의 외부 성기로 구성되어 있습니다(그림 1a 참조). 여기에는 많은 부분이 포함됩니다:
(a) 대음순 - 여성의 내부 성기를 둘러싸고 보호하는 "큰 입술"입니다;
(b) 소음순 - 질과 요도의 입구를 둘러싸고 정의하는 "작은 입술";
(c) 소전정샘과 대전정샘(VG).
소전정샘은 스킨샘(사진에 표시되지 않음)이라고도 하며 질 벽에 있고 여성의 사정과 관련이 있으며 신화적으로 지스팟과 연관되어 있습니다(Kilchevsky et al., 2012; Wickman, 2017). 바르톨린샘이라고도 불리는 주요 VG는 질 좌우에 위치하며 성교를 돕기 위해 윤활유를 생성합니다. 대부분의 여성, 특히 폐경 후 여성은 일생 중 어느 시점에 윤활이 불충분하여 성관계 시 불편함이나 통증을 느낀다고 보고합니다(Nappi & Lachowsky, 2009). 전희 시간을 늘리고 시중에서 판매하는 물, 실리콘 또는 오일 기반 개인 윤활제를 사용하는 것은 이러한 일반적인 문제에 대한 간단한 해결책입니다.
음핵과 질은 외음부의 일부이자 내부 성기로 간주됩니다(그림 1b 참조). 이들은 여성의 쾌락 능력과 관련하여 가장 많이 언급되는 기관입니다(예: Jannini 외, 2012). 평균 전체 흥분 길이가 약 4인치인 18개의 부분으로 구성된 클리토리스의 대부분은 보이지 않습니다(Ginger & Yang, 2011; O'Connell 외., 2005). 눈에 보이는 부분인 귀두와 포피는 요도 위에 위치하며 그 정점에서 소음순과 결합합니다. 음핵은 8,000개 이상의 감각 신경 종말로 구성된 매우 민감하며 오르가즘을 유발하는 데 관여하며, 여성의 90%는 음핵 자극만으로 오르가즘을 느낄 수 있습니다(O'Connell 외., 2005; Thompson, 2016).
"산도"라고도 불리는 질은 자궁경부부터 질 입구까지 이어지는 근육질의 관입니다. 평균 전체 여기 길이는 약 4.5인치이며(Masters & Johnson, 1966), 두 부분으로 나뉩니다: 첫째, 임신 초기에 형성되는 안쪽 3분의 2(후벽)가 있습니다. 둘째, 질의 바깥쪽 1/3(전벽)이 있습니다. 임신 후기에 형성되며 일반적으로 안쪽 부분보다 더 민감하지만 음핵보다는 극적으로 덜 민감합니다 (Hines, 2001). 여성의 10 %에서 30 %만이 질 자극만으로 오르가즘에 도달합니다 (Thompson, 2016). 질의 양쪽 끝에는 자궁경부(자궁의 아래쪽 부분)와 질 입구(몸 바깥쪽으로 열리는 질 입구)가 있습니다. 질은 정자 세포가 들어오고 생리액과 아기가 나가는 통로 역할을 합니다. 건강한 질의 pH는 약 4로 산성입니다. 정상적인 상황(예: 생리, 탐폰 사용, 성관계)으로 인해 pH 수치가 변하면 질 냄새와 통증을 유발하는 미생물의 번식이 용이해집니다(Anderson, Klink & Cohrssen, 2004). 이 잠재적인 문제는 일반의약품 질 젤이나 경구용 프로바이오틱스를 사용하여 정상적인 질 내 pH 수준을 유지함으로써 해결할 수 있습니다(Tachedjiana 외, 논문 발표 중).

여성 내부 생식기의 주요 기능은 난자 세포(난자)를 저장, 운반 및 건강하게 유지하고 호르몬을 생성하는 것입니다(그림 1b 참조). 이러한 기관에는 다음이 포함됩니다:
(a) 자궁(또는 자궁)-출산 전까지 인간의 발달이 이루어지는 곳입니다;
(b) 난소 - 난자(난자, 약 200만 개; Faddy 외, 1992)를 보관하고 프로게스테론, 에스트로겐 및 소량의 테스토스테론을 생성하는 분비샘;
(c) 나팔관 - 수정이 일어날 가능성이 가장 높은 곳입니다. 이 관은 난자가 난소에서 자궁으로 이동하는 배란(약 28일마다)을 허용합니다. 수정이 일어나지 않으면 월경이 시작됩니다. "생리"라고도 하는 월경은 난자가 질을 통해 자궁 내막과 함께 배출되는 것으로, 보통 며칠이 걸립니다.
남성 해부학
남성에게 가장 눈에 띄는 외부 성기는 음경입니다. 음경의 주요 기능은 오르가슴을 유발하고 몸에서 정액과 소변을 운반하는 것입니다. 평균적으로 이완된 음경의 길이는 약 3.5인치인 반면, 발기된 음경의 길이는 약 5인치입니다(Veale et al., 2015; Wessells, Lue & McAninch, 1996). 특정 남성의 발기된 음경의 길이를 알고 싶다면, 발기된 음경의 길이와 (가) 이완된 음경의 길이, (나) 발, 손, 팔뚝, 전체 키 등 다른 신체 부위의 길이, (다) 인종 및 민족 간에는 신뢰할 만한 상관관계가 없기 때문에 실제로 직접 확인해야 합니다(Shah & Christopher, 2002; Siminoski & Bain, 1993; Veale et al, 2015; Wessells, Lue & McAninch, 1996). 음경은 뿌리, 축, 귀두의 세 부분으로 구성됩니다. 포피는 포경수술을 받은 남성을 제외하고 귀두 또는 음경의 머리를 덮고 있습니다. 귀두는 매우 민감하며 4,000개 이상의 감각 신경 종말로 구성되어 있으며 오르가즘을 시작하는 것과 관련이 있습니다(Halata, 1997). 마지막으로, 귀두에는 정액과 소변이 몸 밖으로 빠져나갈 수 있는 요도 입구가 있습니다.

음경 외에도 호르몬과 정자 세포를 생성하는 두 가지 주요 기능을 하는 남성 외부 성 기관이 있습니다. 음낭은 고환이 들어 있는 음경 뒤쪽과 아래쪽의 피부 주머니입니다. 고환(또는 고환)은 테스토스테론, 프로게스테론, 소량의 에스트로겐 및 정자 세포를 생성하는 샘입니다.
많은 사람이 남성에게도 내부 성기가 있다는 사실에 놀라움을 금치 못합니다. 남성 내부 생식기의 주요 기능은 정자 세포를 운반하고, 정자 세포를 건강하게 유지하며, 정자 세포가 운반되는 액체인 정액을 생성하는 것입니다. 남성의 내부 생식기에는 다음이 포함됩니다:
(a) 부고환은 정자 세포를 성숙시키고, 저장하고, 정관으로 운반하는 꼬불꼬불한 관입니다;
(b) 정관 - 정관 수술을 받은 남성을 제외하고 성숙한 정자를 요도로 운반하는 근육 관입니다;
(c) 정낭-정자 세포가 움직일 수 있도록 에너지를 공급하는 분비선. 이 에너지는 설탕(과당) 형태이며 정액의 약 75%를 구성합니다. 정자 세포는 정액의 약 1%만 구성합니다(Owen & Katz, 2005);
(d) 정자 세포에 영양을 공급하는 액체를 정액에 추가로 공급하는 전립선, 요도를 윤활하고 소변으로 인한 산성도를 중화시키는 액체를 생성하는 카우퍼샘이 있습니다;
(e) 요도 - 소변과 정액을 체외로 운반하는 관입니다.
뇌의 섹스

언뜻 보기에도, 만져보기에도 음핵과 음경은 해부학적으로 가장 쾌감을 주는 부위인 것처럼 보입니다. 하지만 이 두 기관은 중추 신경계의 쾌락 수용 능력에 비하면 미미한 수준입니다. 쾌락을 경험할 때 뇌와 뇌간의 광범위한 영역이 활성화되는데, 여기에는 섬, 측두 피질, 변연계, 편도체핵, 기저핵, 상두정피질, 배측 전전두피질, 소뇌 등이 포함됩니다(그림 3 참조, Ortigue 외., 2007). 신경 영상 기술은 환자가 피부를 직접 자극하지 않고 자발적인 오르가즘을 느낄 때(예: Fadul 외, 2005), 실험 참가자가 성감대를 스스로 자극할 때(예: Komisaruk 외, 2011) 뇌의 이러한 영역이 활성화된다는 것을 보여줍니다. 성감대는 신경계를 통해 뇌의 체성감각 피질과 연결된 피부의 민감한 부위입니다.

체성감각피질(SC)은 주로 피부의 감각 정보를 처리하는 뇌의 일부입니다. 피부 부위(예: 입술)가 더 민감할수록 SC의 해당 영역이 커지고, 피부 부위(예: 몸통)가 덜 민감할수록 SC의 해당 영역이 작아집니다(그림 4, Penfield & Boldrey, 1937 참조). 사람의 민감한 신체 부위를 만지면 일반적으로 뇌는 다음 세 가지 중 한 가지 방식으로 해석합니다: "간지럽다!" "아프다!" 또는 "그거...다시 해야 해!" 따라서 우리 몸의 더 민감한 부위일수록 쾌감을 불러일으킬 가능성이 더 큽니다. 누멘마와 그의 동료들이 수행한 연구(2016)에서는 이 가설을 테스트하기 위해 독특한 방법을 사용했습니다. 누멘마 연구팀은 실험 참가자들에게 동성 및 이성의 신체 이미지를 보여주었습니다. 그런 다음 참가자들에게 자신 또는 이성이 자위를 하거나 파트너와 성관계를 가질 때 성적으로 흥분되는 신체 부위를 만졌을 때 색칠하도록 요청했습니다. 그 결과 외부 성기, 유방, 항문 주변에 예상되는 '핫스팟' 성감대가 발견되었지만, 이러한 핫스팟을 넘어서는 피부 부위도 보고되었습니다: "거의 모든 신체 부위의 활동적인 자극은 성적 흥분을 유발합니다...." 또한, 그는 "[핫스팟을 넘어] 파트너와의 섹스는..."..."쌍의 유대감을 유지하는 데있어 만지는 역할을 반영합니다."라고 결론지었습니다.
생리와 성적 반응 주기
뇌와 기타 성 기관은 성적 자극에 대해 성적 반응 주기(SRC; Masters & Johnson, 1966)라는 보편적인 방식으로 반응합니다. SRC는 네 단계로 구성됩니다:
- 흥분: 흥분 단계는 자율신경계의 교감신경이 활성화되어 심박수와 호흡이 빨라지고 음경, 질벽, 음핵, 젖꼭지로 가는 혈류량이 증가합니다. 얼굴 찡그림과 같은 불수의적인 근육 움직임(근긴장)도 이 단계에서 발생합니다.
- 정체기: 정체기: 정체기에는 혈류량, 심박수, 호흡이 강화됩니다. 흔히 "전희"라고도 하는 이 단계에서 여성은 질벽의 바깥쪽 1/3이 조여지는 오르가즘의 플랫폼을 경험하고 남성은 건강한 정자 세포가 포함된 정액 전액을 방출합니다(Killick et al., 2011). 이러한 체액의 조기 방출은 음경 철수를 상대적으로 비효율적인 피임법으로 만듭니다(Aisch & Marsh, 2014). (질문: 금단 피임법을 사용하는 커플을 뭐라고 부르나요? 답변: 부모입니다.)
- 오르가즘: 가장 짧지만 가장 즐거운 단계는 오르가즘 단계입니다. 절정에 도달하면 신경 근육의 긴장이 풀리고 옥시토신 호르몬이 혈류에 넘쳐나면서 정서적 유대감을 촉진합니다. 오르가슴의 리드미컬한 근육 수축은 일시적으로 사정과 관련이 있지만, 오르가슴과 사정은 별개의 생리적 과정이기 때문에 이러한 연관성이 반드시 필요한 것은 아닙니다.
- 해상도: 해결 단계에서는 신체가 각성 전 상태로 돌아갑니다. 남성은 성적 자극에 반응하지 않는 불응기에 들어갑니다. 이 기간의 길이는 나이, 최근 성관계 빈도, 파트너와의 친밀감 수준, 새로움에 따라 달라집니다. 여성은 불응기가 없기 때문에 생리적으로 여러 번의 오르가즘을 경험할 가능성이 더 높습니다. 아이러니하게도 여성은 오르가즘을 '가짜'로 느낄 가능성도 더 높습니다(Opperman 외., 2014).
주목할 점은 자위 행위, 로맨틱 키스, 구강, 질, 항문 성교 등 성행위 유형에 관계없이 SRC가 발생한다는 점입니다(Masters & Johnson, 1966). 또한, 파트너 또는 환경적 대상은 SRC를 발생시키는 데 충분하지만 필수는 아닙니다.
Pregnancy
SRC의 잠재적 결과 중 하나는 임신, 즉 여성이 자궁 내에 태아를 품는 시기입니다. 어떻게 이런 일이 발생하나요?

이 과정은 질 성교 중에 남성이 사정하거나 정액을 방출할 때 시작됩니다. 각 사정에는 약 3억 개의 정자 세포가 포함되어 있습니다. 이 정자는 자궁경부를 통과하여 자궁으로 들어가기 위해 경쟁합니다. 임신은 일반적으로 나팔관 내에서 단일 정자 세포가 난자(난자)와 접촉할 때 발생합니다. 정자는 난자를 수정하기 위해 X-염색체 또는 Y염색체를 가지고 있으며, 난자 자체는 일반적으로 X-염색체를 가지고 있습니다. 이 염색체는 서로 결합하여 사람의 성별을 결정합니다. 두 개의 X 염색체가 결합하면 암컷 접합체(수정란)가 생성됩니다. X 염색체와 Y 염색체의 조합은 남성 접합자를 생성합니다. XX 또는 XY 염색체는 23번째 염색체 세트(대부분의 인간은 총 46개의 염색체를 가지고 있음)를 형성하며, 이를 흔히 염색체 성별 또는 유전적 성별이라고 합니다.
흥미롭게도 1,000명당 1명꼴로 일반적인 XX 또는 XY 세트를 벗어난 염색체 성별의 변이가 발생합니다. 이러한 변형 중 일부에는 XXX, XXY, XYY 또는 단일 X가 포함됩니다(Dreger, 1998). 평균보다 키가 크거나 목이 두껍거나 불임(생식 불능)과 같은 비정상적인 신체적 특징을 가진 경우도 있지만, 대부분의 경우 인지적, 신체적, 성적 문제는 없습니다(Wisniewski 외., 2000). 1,000명 중 거의 15명이 다태아(쌍둥이, 세쌍둥이, 네쌍둥이 등)를 출산합니다. 다태아는 두 가지 방식으로 발생할 수 있습니다. 이질성(이란성) 출산은 한 여성이 여러 개의 난자를 방출하고 그 중 하나 이상이 정자에 의해 수정된 결과입니다. 정자는 X 또는 Y 염색체를 가지고 있기 때문에, 이란성 쌍둥이 출산은 성별의 조합(예: 두 명의 여아 또는 남아와 여아)이 될 수 있습니다. 쌍둥이는 자궁에서 함께 성장하며 보통 몇 분 이내에 태어납니다. 일란성(일란성) 출산은 수정란이 여러 개의 동일한 배아로 분열하여 동시에 발달하는 특수한 상황에서 발생합니다. 따라서 일란성 쌍둥이는 동성입니다.
임신 후 몇 시간이 지나면 접합체는 추가 세포로 분열하기 시작합니다. 그런 다음 나팔관을 따라 내려가 배반포가 되어 자궁에 들어갈 때까지 이동하기 시작합니다. 배반포는 자궁벽에 착상하여 배아가 됩니다(Moore, Persaud & Torchia, 2016). 그러나 성공적인 착상 비율은 여전히 미스터리로 남아 있습니다. 연구자들은 실패율이 60%에 달한다고 보고 있습니다(Diedrich et al., 2007). 실패한 배반포는 월경 중에 제거되며, 여성은 임신이 일어났다는 사실조차 알지 못하는 경우가 많습니다.
산모의 임신 기간은 총 3기로, 마지막 월경부터 시작하여 약 40주 후에 끝나며 각 임신 기간은 13주입니다. 임신 초기에는 태아의 신체 부위가 대부분 형성되지만, 이 단계에서는 출생 시와 같은 비율로 형성되지는 않습니다. 예를 들어, 뇌와 머리는 이 시점에서 신체의 약 절반을 차지합니다. 임신 5 주와 6 주 동안 원시 생식선이 형성됩니다. 그들은 결국 난소 또는 고환으로 발달합니다. 7주까지 발달 중인 배아는 염색체 성별에 관계없이 남성(울피안관) 또는 여성(뮬러관)의 내부 성기를 가질 가능성이 있습니다. 실제로 모든 배아는 Y염색체에 위치한 SRY 유전자가 없는 한 여성 내부 생식기를 갖는 선천적 경향이 있습니다(Grumbach & Conte, 1998; Wizemann & Pardue, 2001). SRY 유전자는 XY 배아가 고환(수질에서 세포를 분열시키는 세포)을 발달하게 합니다. 고환은 남성 내부 생식기인 부고환, 정낭, 정관으로 변하는 울피안 관의 발달을 자극하는 테스토스테론을 방출합니다. 고환은 또한 뮬러관을 위축시키는 호르몬인 뮬러관 억제 물질을 방출합니다. SRY 유전자가 존재하지 않거나 활성화되지 않는 경우(염색체 암컷(XX)의 전형적인 경우), XX 배아는 난소(피질에서 세포 분열)가 발달하고 뮬러관은 나팔관, 자궁, 자궁경부 및 질의 안쪽 2/3를 포함한 여성 내부 성기관으로 변모합니다(Carlson, 1986). 고환에서 테스토스테론이 분비되지 않으면 울리안 관은 자연적으로 기능이 저하됩니다(Grumbach & Conte, 1998; Wizemann & Pardue, 2001).
임신 후반기에 임산부는 자궁의 움직임을 느낄 수 있습니다. 이를 태동이라고 합니다. 자궁 안에서 태아는 몸 전체에 가는 털(라누고)과 속눈썹, 눈썹이 발달합니다. 췌장과 간과 같은 주요 장기가 완전히 기능하기 시작합니다. 임신 20 주가되면 외부 성기가 완전히 형성되기 때문에이 기간 동안 초음파를 사용한 "성별 결정"이 임신 초기에 비해 더 정확합니다 (Igbinedion & Akhigbe, 2012; Odeh, Ophir & Bornstein, 2008). 남성 외부 성기(예: 음경 및 음낭)의 형성은 높은 수준의 테스토스테론에 의존하는 반면, 여성 외부 성기(예: 질 바깥쪽 1/3 및 클리토리스)는 호르몬의 영향 없이 형성됩니다(Carlson, 1986). 에스트로겐, 테스토스테론, 프로게스테론과 같은 성 호르몬 수치는 이 임신 기간 동안 뇌에 영향을 미치기 시작하여 성 정체성 및 성적 지향과 관련된 미래의 감정, 행동 및 사고에 영향을 미칩니다(Swaab, 2004). 이 발달 단계에서 염색체 성, 생식선 성, 성 호르몬, 내부 성기, 외부 성기 및 뇌 분화의 상호 작용은 너무 복잡하여 역사적으로 사람을 설명하는 데 사용되어 온 익숙한 성, 성별 및 성적 지향 범주에 쉽게 부합하지 않는다는 점을 이해하는 것이 중요합니다(Herdt, 1996). 임신 후반기 말, 즉 약 26주가 되면 자궁 밖에서 생존할 확률이 90% 이상인 생존 가능 시기가 됩니다(Rysavy 외., 2015). 흥미롭게도 기술 발전과 병원 치료의 변화가 생존 가능 연령에 영향을 미쳐 임신 초기에 생존이 가능해졌습니다(Rysavy et al., 2015).

임신 3개월 동안에는 뇌가 빠르게 발달하고 체중이 급격히 증가합니다. 일반적으로 36주가 되면 태아가 머리부터 자궁강으로 내려오기 시작합니다. 출산 준비만이 임신 말기에 나타나는 유일한 행동은 아닙니다. 이 시기에는 남성 태아의 발기 반응이 나타나며(Haffner, 1999; Martinson, 1994; Parrot, 1994), Giorgi와 Siccardi(1996)는 태아가 외부 성기를 스스로 탐색하는 모습을 초음파로 관찰한 결과를 보고했습니다. 대부분의 아기는 질식 분만(질을 통해)으로 태어나지만 미국에서는 1/3이 제왕절개(복부를 통해)로 태어납니다(Molina et al., 2015). 신생아의 건강은 처음에는 체중(보통 2,500~4,000g)에 따라 결정되지만, 출생 체중은 인종에 따라 크게 다릅니다(Jannsen 외., 2007).
피임
피임 또는 피임법은 성관계로 인한 임신 확률을 줄여줍니다. 피임에는 호르몬 피임법, 장벽 피임법, 자연 피임법 등 다양한 형태가 있습니다. 표 1에서 볼 수 있듯이, 다양한 피임법의 효과는 68%에서 99.9%까지 매우 다양합니다(optionsforsexualhealth.org).
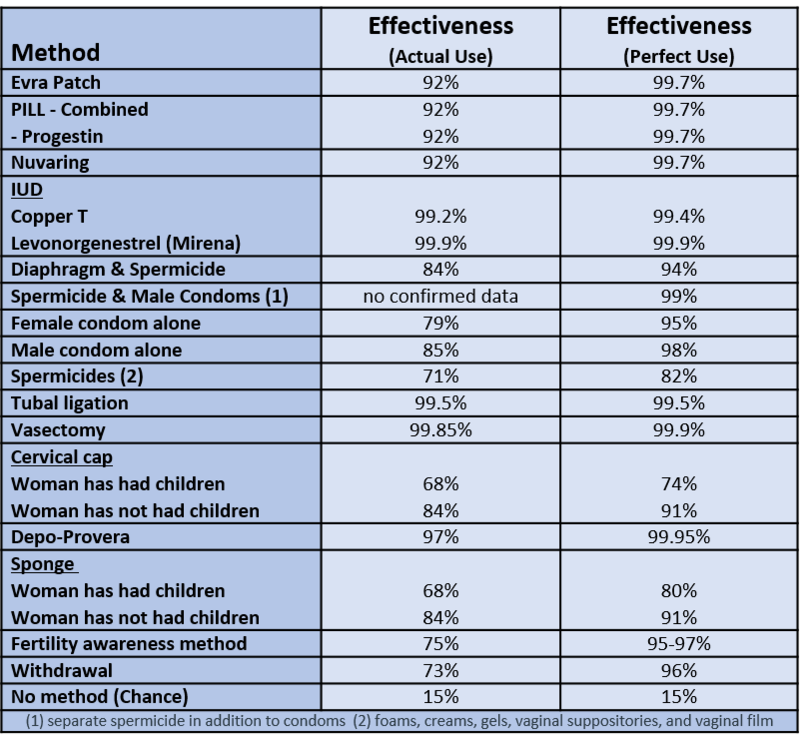
호르몬 형태의 피임법은 합성 에스트로겐 또는 프로게스틴을 방출하여 배란을 방지하고 자궁 경부 점액을 두껍게 만들어 정자가 난자에 도달하기 어렵게 만듭니다(sexandu.ca/contraception). 이러한 호르몬을 체내에 도입하는 방법에는 이식형 막대, 피임약, 주사, 경피 패치, IUD, 질 링 등 다양한 방법이 있습니다. 예를 들어, 질 링은 92%의 피임 효과가 있으며, 사용자가 질에 쉽게 삽입하고 뺄 수 있고, 얇은 플라스틱으로 구성되어 있으며, 보통 약 3주 동안 질에 머무는 동안 방출되는 호르몬의 조합으로 구성되어 있습니다.
장벽 형태의 피임법은 정자에 독성이 있는 물리적 장벽 또는 화학적 장벽을 만들어 정자가 자궁으로 들어가는 것을 방지합니다. 정관 수술, 난관 결찰, 남성용 및 여성용 콘돔, 살정제, 횡경막, 자궁경부 캡 등 다양한 차단 방법이 있습니다. 가장 많이 사용되는 차단 방법은 콘돔으로, 79~85%의 피임 효과가 있습니다. 남성용 콘돔은 음경 위에 착용하는 반면, 여성용 콘돔은 질 내부에 착용하여 자궁경부 주위를 감싸는 방식입니다. 콘돔은 체액 교환을 방지하고 피부와 피부의 접촉을 줄여줍니다. 이러한 이유로 콘돔은 일부 성병(STI)의 위험을 줄이기 위해 사용되기도 합니다. 그러나 콘돔을 여러 개 착용하면 마찰로 인해 미세한 찢김이 발생하여 콘돔의 효과가 떨어지므로 삽입 시 남녀 콘돔 또는 두 개의 콘돔을 동시에 착용해서는 안 된다는 점에 유의해야 합니다(Munoz, Davtyan & Brown, 2014).
자연적인 형태의 피임법은 생리 주기에 대한 지식과 신체에 대한 인식에 의존합니다. 여기에는 가임력 인식법(FAM), 수유기 무월경법, 금욕법 등이 포함됩니다. 예를 들어, FAM의 효과는 약 75%이며, 생리 주기를 추적하고 여성의 가임 기간 동안 성관계를 피하거나 다른 형태의 피임법을 사용해야 합니다. 여성의 가임 기간(임신 가능성이 가장 높은 기간)의 약 30%는 생리 주기 중 10일에서 17일 사이에 해당합니다(Wilcox, Dunson & Baird, 2000). 나머지 70%의 여성은 불규칙하고 예측하기 어려운 가임 기간을 경험하기 때문에 FAM의 효과가 감소합니다.
위의 범주에 속하지 않는 다른 형태의 피임법으로는 응급 피임약, 구리 IUD, 금욕 등이 있습니다. 응급 피임약(예: 플랜 B)은 배란 전에 복용하면 난자의 방출을 지연시킵니다. 응급 피임은 일반적으로 무방비 성관계, 콘돔 사고 또는 성폭행 후에 사용하는 피임법입니다. 가장 효과적인 응급 피임법은 구리 IUD입니다. 의료 전문가가 자궁경부 개구부를 통해 자궁에 IUD를 삽입합니다. 99% 이상의 피임 효과가 있으며 10년 이상 자궁 내에 남아있을 수 있습니다. 호르몬이 없고 구리 이온을 사용하여 정자가 살기 어려운 환경을 조성하여 수정 가능성을 크게 낮추기 때문에 일반적인 IUD와 다릅니다. 또한 구리 이온은 자궁 내막을 변화시켜 착상 가능성을 크게 감소시킵니다. 마지막으로, 임신으로 이어질 수 있는 모든 성행위를 피하는 금욕은 100% 피임 성공률을 가진 유일한 피임법입니다.
특정 개인에게 가장 적합한 피임 방법을 결정하는 데는 여러 가지 요인이 있습니다. 일부 요인은 성격 및 습관과 관련이 있습니다. 예를 들어, 건망증이 있는 여성에게는 매일 복용해야 하는 피임약이 최선의 선택이 아닐 수 있습니다. 피임 선택에 영향을 미치는 다른 요인으로는 비용, 나이, 교육, 종교적 신념, 라이프스타일, 성 건강 등이 있습니다.
성병 감염
안타깝게도 성행위의 잠재적 결과는 감염입니다. 성병은 다른 전염성 감염병과 비슷하지만, 성병은 주로 사회적 성행위를 통해 전염된다는 점이 다릅니다. 사회적 성행위에는 로맨틱한 키스와 구강, 질, 항문 성교가 포함됩니다. 또한 성병은 혈액을 통해, 그리고 임신과 출산 중에 산모와 아이 사이에 전염될 수 있습니다. 성병은 성병(STD)으로 이어질 수 있습니다. 종종 감염은 증상이 없으며 질병으로 이어지지 않습니다. 예를 들어, 미국에서 남성과 여성에게 가장 흔한 성병은 인유두종 바이러스(HPV)입니다. 대부분의 경우 HPV는 저절로 사라지고 증상이 없습니다. HPV 성병의 일부만이 자궁경부암, 음경암, 구강암 또는 인후암으로 발전합니다(미국 질병통제예방센터, CDCP, 2016년 12월).
성병은 30가지가 넘습니다. 성병은 주요 전염 방법, 증상, 치료법, 바이러스 또는 박테리아로 인한 것인지 여부가 다릅니다. 전 세계적으로 가장 흔한 성병은 생식기 헤르페스(5억 명), HPV(2억 9천만 명), 트리코모나스(1억 4천 3백만 명), 클라미디아(1억 3천 1백만 명), 임질(7천 8백만 명), 인간 면역결핍 바이러스(HIV, 3천 6백만 명), 매독(6백만 명; 세계보건기구, 2016) 등입니다.
성병 감염 여부를 확인하기 위한 의료 검사는 비교적 간단하고 무료인 경우가 많습니다(gettested.cdc.gov). 또한 모든 성병에 대한 백신이나 치료제가 있으며, 많은 성병(예: 클라미디아, 임질, 트리코모나스증)은 치료할 수 있습니다. 그러나 치료를 받지 않으면 모든 성병은 일부 성병으로 인한 사망을 포함하여 잠재적으로 건강에 부정적인 영향을 미칠 수 있습니다. 예를 들어, HIV는 치료하지 않으면 후천성면역결핍증후군(AIDS)으로 이어지는 경우가 많으며, 매년 백만 명이 넘는 사람들이 AIDS로 사망합니다(aids.gov). 안타깝게도 성병 감염자 대부분은 아니더라도 많은 사람들이 검사나 치료를 받지 않습니다. 예를 들어, HIV 감염자의 30%, 생식기 헤르페스 감염자의 90%가 성병에 걸렸다는 사실을 모르고 있습니다(플레밍 외, 1997; 응우옌 & 홀로드니, 2008).

성병에 걸리지 않은 사람으로부터 성병에 감염되는 것은 불가능합니다. 당연한 말처럼 보일 수 있지만, 최근 한 연구에서 대학생 1학년과 2학년 596명에게 "파트너가 에이즈 바이러스에 감염되지 않았더라도 항문(직장) 성교를 하면 에이즈에 걸릴 수 있다"는 참/거짓 질문을 던진 결과 33%가 "그렇다"고 답했습니다(Lucas et al., 2016). 분명한 것은 항문 성교가 에이즈를 유발한다는 잘못된 고정관념이 우리의 집단적 성 지식에 잘못된 정보를 계속 제공하고 있다는 것입니다. 인간의 성에 대한 개방적이고 정직하며 포괄적인 교육만이 이러한 성병 고정관념에 맞서 싸울 수 있습니다. 명확히 말하자면, 항문 성교는 성병과 관련이 있지만 성병을 유발할 수는 없습니다. 특히 항문 성교는 질 성교(두 번째로 전염 가능성이 높은 방법), 구강 성교(세 번째로 전염 가능성이 높은 방법), 로맨틱 키스(네 번째로 전염 가능성이 높은 방법)와 비교할 때 직장 내벽이 상대적으로 얇고 찢어지고 출혈이 발생하여 감염을 전염시키기 쉽기 때문에 성병 전염 및 감염 위험이 가장 큰 것으로 알려져 있습니다(CDCP, 2016).
성적으로 활동적인 사람이 성병에 걸릴 확률은 다양한 요인에 따라 달라집니다. 그 중 두 가지 요인은 나이와 성교육 접근성입니다. 15세에서 24세 사이의 젊은이들은 성적으로 활동적인 인구의 약 25%에 불과하지만 전체 신규 성병의 50% 이상을 차지합니다(Satterwhite 외., 2013). 일반적으로 젊은 남성과 여성은 똑같이 성병에 걸리기 쉽지만, 여성이 성병으로 인한 장기적인 건강상의 후유증을 겪을 가능성이 훨씬 더 높습니다. 예를 들어, 미국에서는 매년 진단되지 않은 성병으로 인해 약 24,000명의 여성이 불임에 시달리고 있습니다(CDCP, 2016년 10월; DiClemente, Salazar & Crosby, 2007).
포괄적인 성교육에 대한 접근성이 제한되어 있는 것도 성병에 걸릴 위험을 높이는 주요 요인입니다. 안타깝게도 일부 성교육은 금욕 장려에 국한되어 있으며 "순결 서약"에 크게 의존하고 있습니다. 순결 서약은 이성애 결혼 전까지 성관계를 자제하겠다는 서약입니다. 순결 서약은 일부 문화적, 종교적 세계관에 잘 맞지만, 실제로 금욕을 유지하는 경우에만 효과적입니다. 안타깝게도 항상 그런 것은 아니며, 연구에 따르면 이러한 유형의 전략이 역효과를 낼 수 있는 여러 가지 방법이 밝혀졌습니다. 순결 서약을 한 청소년은 성생활을 시작했을 때 피임법을 사용할 가능성이 다른 청소년에 비해 현저히 낮습니다(Bearman & Brückner, 2001). 또한, 순결 서약자는 비서약자보다 구강 성교와 항문 성교를 모두 할 가능성이 4~6배 더 높으며(Paik, Sanchagrin & Heimer, 2016), 단순히 질 성교를 피함으로써 처녀성을 지키고 있다고 생각하는 경우가 많습니다. 실제로 순결 서약을 하는 학생이 있는 학교는 그렇지 않은 학교보다 성병 발생률이 훨씬 높습니다(Bearman & Brückner, 2001).
흥미롭게도 노인은 유럽과 미국에서 성병 진단을 받는 인구 중 가장 빠르게 증가하는 계층 중 하나입니다. 미국 질병통제예방센터에 따르면 65세 이상에서 HIV 진단을 받은 사람이 꾸준히 증가하고 있으며, 2007년 이후 노년층의 매독 발생률은 52%, 클라미디아는 32% 증가했고, 2010년부터 2014년까지 50세에서 70세 사이의 STI 진단은 38% 증가했습니다(Forster, 2016; Weiss, 2014). 왜 이런 일이 일어나고 있을까요? 노인이 청소년보다 성에 대해 더 잘 알고 있는 것은 아니며, 젊은 사람보다 포괄적인 성교육에 대한 접근성이 떨어질 수 있다는 점을 명심하세요(Adams, Oye & Parker, 2003). 그럼에도 불구하고 의학의 발전으로 인해 노년층도 노년기에도 성생활을 계속할 수 있으며, 청소년과 마찬가지로 안전한 성관계에 대해 실수할 수 있습니다.
더 안전한 성관계
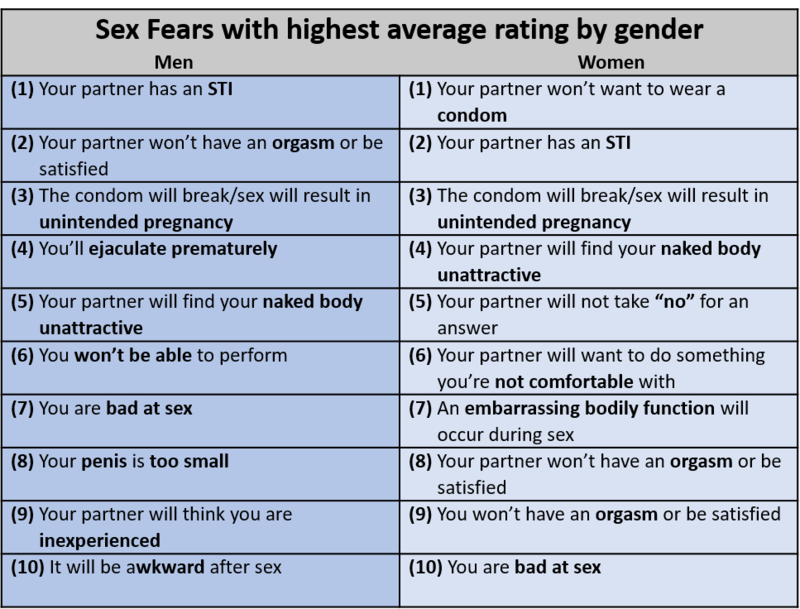
성병은 100% 예방할 수 있습니다: 사교적인 성행위를 하지 않기만 하면 됩니다. 하지만 큰 틀에서 보면 성관계를 피하는 것이 신체적, 정신적 건강에 해롭다는 사실에 놀랄 수도 있지만, 오히려 성관계는 건강에 많은 도움이 될 수 있습니다(Charnetski & Brennan, 2004; Ditzen, Hoppmann & Klumb, 2008; Hall et al., 2010). 따라서 트위터에서는 의사소통, 정직성, 차단 방법과 같은 보다 안전한 성관계 관행을 권장합니다. 안전한 성관계 관행은 항상 소통에서 시작됩니다. 파트너와 성행위를 하기 전에 자신과 파트너의 경계에 대해 명확하고 정직하며 명시적으로 이해해야 합니다. 보다 안전한 섹스를 위해서는 특정 성행위와 관련된 장벽(남성용 콘돔, 여성용 콘돔 또는 치과용 댐)에 대해 논의하고 사용하는 것이 포함됩니다. 또한 명심하세요: 안전한 성관계는 피임과 동일한 도구를 일부 사용할 수 있지만, 안전한 성관계는 피임이 아닙니다. 피임은 생식에 중점을 두지만, 안전한 성관계는 웰빙에 중점을 둡니다. 성적인 행동에 대한 적극적인 접근 방식은 처음에는 부담스러워 보일 수 있지만, '전희'로 쉽게 상상할 수 있으며, 성적 만족도를 높이고 오르가즘을 느낄 확률을 높이며 성관계 시 느끼는 두려움을 해소할 수 있습니다(표 2 참조; Jalili, 2016; Nuno, 2017).
성기능 장애
여성의 약 43%와 남성의 약 31%가 SRC에 명시된 대로 성적 쾌감이나 반응성을 경험하는 능력에 임상적으로 심각한 장애를 겪고 있습니다(Rosen, 2000). 정신장애 진단 및 통계 편람 5판(DSM)에서는 이러한 어려움을 성기능 장애라고 부릅니다.
DSM에 따르면 남성 특유의 성기능 장애에는 네 가지가 있습니다:
- 사정 지연
- 발기 장애(ED)
- 남성 저활동성 성욕 장애
- 조루(PE)
세 가지 여성 특유의 기능 장애가 있습니다:
- 여성 오르가즘 장애
- 여성 성적 관심/각성 장애
- 생식기-골반 통증/침투 장애
성별에 국한되지 않는 성기능 장애로는 약물/약물에 의한 성기능 장애도 있습니다(미국 정신의학 협회, 2013). 가장 흔하게 보고되는 남성 성기능 장애는 조루(PE)와 발기 부전(ED)인 반면, 여성은 욕망과 각성과 관련된 성기능 장애를 가장 자주 보고합니다. 또한 여성은 여러 가지 성기능 장애를 경험할 가능성이 더 높습니다(McCabe et al., 2016).
조루증은 성기능을 손상시키고 개인적인 고통을 유발하는 조기 사정 패턴입니다. 심한 경우 성행위 시작 전 또는 삽입 후 15초 이내에 사정이 발생할 수 있습니다(미국 정신과 협회, 2013). 발기 부전은 유병률이 20~30%에 이르는 매우 흔한 성기능 장애입니다. 관계 및 친밀감의 어려움, 불안, 낮은 자신감, 우울증은 종종 발기 부전증과 관련이 있습니다. 대부분의 발기 부전 남성은 치료를 받지 않습니다(Porst et al., 2007).
발기 부전은 발기를 얻거나 유지하기가 자주 어렵거나 발기 강직도가 현저히 감소하는 것을 말합니다. 정상적인 노화는 특히 50세 이후에 발기 부전의 유병률과 발생률을 증가시킵니다(미국 정신과 협회, 2013). 그러나 최근 연구에 따르면 30세 미만의 젊은 남성에서 발기부전 유병률이 크게 증가하는 것으로 나타났습니다(예: Capogrosso 외., 2013).
여성 성적 관심/각성 장애(FSIAD)는 성적 관심이나 각성이 감소하거나 없는 것이 특징입니다. FSIAD 진단을 받은 사람은 다음 감정, 행동, 사고 중 세 가지 이상이 6개월 이상 지속됩니다:
- 성행위에 대한 관심
- 성적 또는 에로틱한 생각과 환상
- 성행위 시작
- 성행위 중 성적 흥분 또는 즐거움
- 성적 또는 에로틱한 신호에 대한 성적 관심/흥분
- 성행위 중 생식기 또는 비생식기 감각
음경-질 성교가 항상 오르가즘을 유발한다는 잘못된 기대와 같이 증상이 불충분한 자극이나 성 지식 부족의 결과인 경우에는 FSIAD로 진단하지 않습니다(미국 정신의학회, 2013).
치료
성기능 장애 치료와 관련하여 좋은 소식과 나쁜 소식이 있습니다. 좋은 소식은 대부분의 성기능 장애에는 치료법이 있지만, 대부분의 사람들이 치료법을 찾지 않는다는 것입니다(Gott & Hinchliff, 2003). 따라서 좋은 소식은 이 모듈에서 배운 지식을 바탕으로 성기능 장애를 경험하고 있다면 치료를 받는 것은 선택의 문제일 뿐이라는 것입니다. 안타깝게도 나쁜 소식은 대부분의 성기능 장애 치료법이 문제의 심리적, 사회문화적 근간을 다루지 않고 생리적 근원에만 초점을 맞춘다는 것입니다. 예를 들어, Montague 등(2007, 1-7쪽)은 미국 비뇨기과학회의 발기부전 치료 옵션에서 "현재 발기부전 치료를 위해 사용할 수 있는 치료법에는 경구용 포스포디에스테라제 5형 억제제, 요도 내 알프로스타딜, 해면체 내 혈관 활성 약물 주사, 진공 수축 장치, 음경 보형물 삽입술 등이 있습니다."라고 명확하게 설명합니다.

생물학적 치료로 증상을 관리하는 데만 초점을 맞춘 치료법은 심리적, 관계적, 사회적 맥락에 기반한 성기능 장애의 근본적인 문제를 소홀히 합니다. 예를 들어, 성관계 중 윤활이 제대로 되지 않아 치료를 받으려는 여성은 증상을 완화하기 위해 보조 윤활제를 처방받을 가능성이 높습니다. 다음에 성관계를 가질 때 윤활유는 질 건조증을 해결할 수 있지만 파트너 학대로 인한 자연적인 각성과 윤활 부족은 완전히 간과됩니다 (Kleinplatz, 2012).
성기능 장애와 관련된 요인에는 관계 문제, 부정적인 성적 태도 및 신념, 의학적 문제, 성적으로 억압적인 문화적 태도, 규범 또는 법률, 일반적인 지식 부족 등 여러 가지가 있습니다. 따라서 성기능 장애에 대한 치료는 문제의 생리적, 심리적, 사회문화적 근원을 해결해야 합니다.
결론
이 모듈의 정보가 여러분의 신체적, 심리적, 관계적 건강에 긍정적인 영향을 미치기를 바랍니다. 처음에 약속드린 대로, 이제 성 해부학과 생리학에 대한 과학적 기초를 습득했으니 은밀한 Google 검색은 줄어들 것입니다. 앞서 언급하지 않은 점은 이러한 기반이 성에 대한 공개적인 Google 검색을 크게 증가시킬 수 있다는 것입니다! 인간의 섹슈얼리티를 탐구하는 것은 무한한 사업입니다. 여러분이 타고난 호기심과 성 지식을 받아들인다면 성에 대한 이해의 여정은 이제 막 시작되었다고 생각합니다.
Acknowledgements
The authors are indebted to Robert Biswas-Diener, Trina Cowan, Kara Paige, and Liz Wright for editing drafts of this module.
Outside Resources
- Journal: The Journal of Sex Research
- http://www.sexscience.org/journal_of_sex_research/
- Journal: The Journal of Sexual Medicine
- http://www.jsm.jsexmed.org/
- Organization: Advocates for Youth partners with youth leaders, adult allies, and youth-serving organizations to advocate for policies and champion programs that recognize young people’s rights to honest sexual health information; accessible, confidential, and affordable sexual health services; and the resources and opportunities necessary to create sexual health equity for all youth.
- http://www.advocatesforyouth.org/
- Organization: SIECUS - the Sexuality Information and Education Council of the United States - was founded in 1964 to provide education and information about sexuality and sexual and reproductive health.
- http://www.siecus.org/
- Organization: The Guttmacher Institute is a leading research and policy organization committed to advancing sexual and reproductive health and rights in the United States and globally.
- https://www.guttmacher.org/
- Video: 5MIweekly—YouTube channel with weekly videos that playfully and scientifically examine human sexuality.
- https://www.youtube.com/channel/UCQFQ0vPPNPS-LYhlbKOzpFw
- Video: Sexplanations—YouTube channel with shame-free educational videos on everything sex.
- https://www.youtube.com/user/sexplanations
- Video: YouTube - AsapSCIENCE
- https://www.youtube.com/user/AsapSCIENCE
- Web: Kinsey Confidential—Podcast with empirically-based answers about sexual questions.
- http://kinseyconfidential.org/
- Web: Sex & Psychology Web: Sex & Psychology—Blog about the science of sex, love, and relationships.
- http://www.lehmiller.com/
Discussion Questions
- Consider your own source(s) of sexual anatomy and physiology information previous to this module. Discuss at least three of your own prior sexual beliefs challenged by the content of this module.
- Pretend you are tasked with teaching a group of adolescents about sexual anatomy, but with a twist: You must teach through the lens of pleasure instead of reproduction. What would your talking points be? Be sure to incorporate the role of the brain in evoking sexual pleasure.
- Given how universal and similar the sexual response cycle is for both males and females, why do you think males enter a refractory period during the resolution phase and females do not? Consider potential evolutionary reasons for why this occurs.
- Imagine yourself as a developing human being from conception to birth. Using a first-person point of view, create a commentary that addresses the significant milestones achieved in each trimester.
- Pretend your hypothetical adolescent daughter has expressed interest in birth control. During her appointment with a health care provider, what are some factors that should be considered prior to selecting the best birth control method for her?
- Describe at least three ways you can reduce your chances of contracting a sexually transmitted infection.
- How can practicing safer sex enhance your well-being?
- As discussed within the module, numerous influences contribute to the development and maintenance of a sexual dysfunction, such as, adverse sexual attitudes and beliefs. Which influences, if any, can you relate to? How do you plan on addressing those influences to achieve optimal sexual health?
Vocabulary
- Abstinence
- Avoiding any sexual behaviors that may lead to conception.
- Age of viability
- The age at which a fetus can survive outside of the uterus.
- Barrier forms of birth control
- Methods in which sperm is prevented from entering the uterus, either through physical or chemical barriers.
- Cervix
- The lower portion of the uterus that connects to the vagina.
- Chromosomal sex
- Also known as genetic sex; defined by the 23rd set of chromosomes.
- Clitoris
- A sensitive and erectile part of the vulva; its main function is to initiate orgasms.
- Conception
- Occurs typically within the fallopian tube, when a single sperm fertilizes an ovum cell.
- Cowper's glands
- Glands that produce a fluid that lubricates the urethra and neutralizes any acidity due to urine.
- Emergency contraception
- A form of birth control used in a variety of circumstances, such as after unprotected sex, condom mishaps, or sexual assault.
- Epididymis
- A twisted duct that matures, stores, and transports sperm cells into the vas deferens.
- Erogenous zones
- Highly sensitive areas of the body.
- Excitement phase
- The activation of the sympathetic branch of the autonomic nervous system defines this phase of the sexual response cycle; heart rate and breathing accelerate, along with increased blood flow to the penis, vaginal walls, clitoris, and nipples.
- Fallopian tubes
- The female’s internal sex organ where fertilization is most likely to occur.
- Foreskin
- The skin covering the glans or head of the penis.
- Glans penis
- The highly sensitive head of the penis, associated with initiating orgasms.
- Hormonal forms of birth control
- Methods by which synthetic estrogen or progesterone are released to prevent ovulation and thicken cervical mucus.
- Introitus
- The vaginal opening to the outside of the body.
- Labia majora
- The “large lips” enclosing and protecting the female internal sex organs.
- Labia minora
- The “small lips” surrounding and defining the openings of the vagina and urethra.
- Menstruation
- The process by which ova as well as the lining of the uterus are discharged from the vagina after fertilization does not occur.
- Mullerian ducts
- Primitive female internal sex organs.
- Myotonia
- Involuntary muscular movements, such as facial grimaces, that occur during the excitement phase of the sexual response cycle.
- Natural forms of birth control
- Methods that rely on knowledge of the menstrual cycle and awareness of the body.
- Neuroimaging techniques
- Seeing and measuring live and active brains by such techniques as electroencephalography (EEG), computerized axial tomography (CAT), and functional magnetic resonance imaging (fMRI).
- Orgasm phase
- The shortest, but most pleasurable, phase of the sexual response cycle.
- Orgasmic platform
- The tightening of the outer third of the vaginal walls during the plateau phase of the sexual response cycle.
- Ovaries
- The glands housing the ova and producing progesterone, estrogen, and small amounts of testosterone.
- Ovulation
- When ova travel from the ovaries to the uterus.
- Oxytocin
- A neurotransmitter that regulates bonding and sexual reproduction.
- Penis
- The most prominent external sex organ in males; it has three main functions: initiating orgasm, and transporting semen and urine outside of the body.
- Plateau phase
- The phase of the sexual response cycle in which blood flow, heart rate, and breathing intensify.
- Plethysmography
- The measuring of changes in blood - or airflow - to organs.
- Pregnancy
- The time in which a female carries a developing human within her uterus.
- Primitive gonads
- Reproductive structures in embryos that will eventually develop into ovaries or testes.
- Prostate gland
- A male gland that releases prostatic fluid to nourish sperm cells.
- Quickening
- The feeling of fetal movement.
- Refractory period
- Time following male ejaculation in which he is unresponsive to sexual stimuli.
- Resolution phase
- The phase of the sexual response cycle in which the body returns to a pre-aroused state.
- Safer-sex practices
- Doing anything that may decrease the probability of sexual assault, sexually transmitted infections, or unwanted pregnancy; these may include using condoms, honesty, and communication.
- Scrotum
- The sac of skin behind and below the penis, containing the testicles.
- Semen
- The fluid that sperm cells are transported within.
- Seminal vesicles
- Glands that provide sperm cells the energy that allows them to move.
- Sexual dysfunctions
- A range of clinically significant impairments in a person’s ability to experience pleasure or respond sexually as outlined by the sexual response cycle.
- Sexual response cycle
- Excitement, Plateau, Orgasm, and Resolution.
- Sexually transmitted infections (STIs)
- Infections primarily transmitted through social sexual behaviors.
- Skene’s glands
- Also called minor vestibular glands, these glands are on the anterior wall of the vagina and are associated with female ejaculation.
- Somatosensory cortex
- A portion of the parietal cortex that processes sensory information from the skin.
- Testicles
- Also called testes—the glands producing testosterone, progesterone, small amounts of estrogen, and sperm cells.
- Trimesters
- Phases of gestation, beginning with the last menstrual period and ending about 40 weeks later; each trimester is roughly 13 weeks in length.
- Urethra
- The tube that carries urine and semen outside of the body.
- Uterus
- Also called the womb—the female’s internal sex organ where offspring develop until birth.
- Vagina
- Also called the birth canal—a muscular canal that spans from the cervix to the introitus, it acts as a transport mechanism for sperm cells coming in, and menstrual fluid and babies going out.
- Vas deferens
- A muscular tube that transports mature sperm to the urethra.
- Vasectomy
- A surgical form of birth control in males, in which the vas deferens is intentionally damaged.
- Vestibular glands (VGs)
- Also called major vestibular glands, these glands are located just to the left and right of the vagina, and produce lubrication to aid in sexual intercourse.
- Vulva
- The female’s external sex organs.
- Wolffian ducts
- Primitive male internal sex organs.
- Zygote
- Fertilized ovum.
References
- Adams, M., S., Oye, J., & Parker, T. S. (2003). Sexuality of older adults and the Internet: From sex education to cybersex. Sexual and Relationship Therapy, 18, 405-415.
- Aisch, G., & Marsh, B. (2014). How Likely Is It That Birth Control Could Let You Down?https://www.nytimes.com/interactive/2014/09/14/sunday-review/unplanned-pregnancies.html. Retrieved on March 23, 2017.
- American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Washington, DC: Author.
- Anderson, M. R., Klink, K., & Cohrssen, A. (2004). Evaluation of vaginal complaints. Journal of The American Medical Association, 291, 1368-1379.
- Bearman, P. S., & Brückner, H. (2001). Promising the future: Virginity pledges and first intercourse. American Journal of Sociology, 106, 859-912.
- Buhi, E.R., Daley, E.M., Oberne, A., Smith, S.A., Schneider, T., Fuhrmann, H.J.(2010). Quality and accuracy of sexual health information web sites visited by young people. Journal of Adolescent Health, Volume 47, Issue 2 , 206 - 208.
- Capogrosso, P., Colicchia, M., Ventimiglia, E., Castagna, G., Clementi, M. C., Suardi, N., Castiglione, F., Briganti, A., Cantiello, F., Damiano, R., Montorsi, F., & Salonia, A. (2013). One patient out of four with newly diagnosed erectile dysfunction is a young man—worrisome picture from the everyday clinical practice. Journal of Sexual Medicine, 10, 1833-1841.
- Carlson, N. R. (1986). Physiology of behavior. Boston: Allyn and Bacon.
- Centers for Disease Control and Prevention (2016). Anal sex and HIV risk. https://www.cdc.gov/hiv/risk/analsex.html Retrieved on March 21, 2017.
- Centers for Disease Control and Prevention (December 2016). What is HPV? https://www.cdc.gov/hpv/parents/whatishpv.html Retrieved on May 6, 2017.
- Centers for Disease Control and Prevention (October 2016). Sexually transmitted disease surveillance, 2015. https://www.cdc.gov/std/stats15/std-surveillance-2015-print.pdf Retrieved on May 6, 2017.
- Centers for Disease Control, National HIV, STD, and Hepatitis Testing.
- Charnetski, C. J., & Brennan, F. X. (2004). Sexual frequency and salivary Immunoglobulin A (IgA). Psychological Reports, 94, 839-844.
- DiClemente, R. J., Salazar, L. F., & Crosby, R. A. (2007). A review of STD/HIV preventive interventions for adolescents: Sustaining effects using an ecological approach. Journal of Pediatric Psychology, 32, 888-906.
- Diedrich, K., Fauser, B. C. J. M., Devroey, P., & Griesinger, G. (2007). The role of the endometrium and embryo in human implantation. Human Reproduction Update, 13, 365-377.
- Ditzen, B., Hoppmann, C., & Klumb, P. (2008). Positive couple interactions and daily cortisol: On the stress-protecting role of intimacy. Psychosomatic Medicine, 70, 883-889.
- Dreger, A. (1998). Ambiguous sex—or ambivalent medicine? Ethical issues in the treatment of intersexuality. Hastings Center Report, 28, 24-35.
- Faddy, M.J., Gosden, R. G., Gougeon, A., Richardson, S. J., & Nelson, J. F. (1992). Accelerated disappearance of ovarian follicles in mid-life: Implications for forecasting menopause. Human Reproduction, 7, 1342–1346.
- Fadul, C. E., Stommel, E. W., Dragnev, K. H., Eskey, C. J., & Dalmau, J. O. (2005). Focal paraneoplastic limbic encephalitis presenting as orgasmic epilepsy. Journal of Neuro Oncology, 72, 195–198.
- Fleming, D. T., et al. (1997). Herpes simplex virus type 2 in the United States, 1976–1994. New England Journal of Medicine, 337, 1105–1111.
- Forster, K. (December 8, 2016). STIs in people aged 50 to 70 have risen by more than a third over the last decade. Independent. http://www.independent.co.uk/life-style/health-and-families/health-news/older-people-stis-sexually-transmitted-infections-50-to-70-chief-medical-officer-report-dame-sally-a7463861.html Retrieved on May 9, 2017.
- Fuxman, S., De Los Santos, S., Finkelstein, D., Landon, M. K., & O’Donnell, L. (2015). Sources of information on sex and antecedents of early sexual initiation among urban Latino youth. American Journal of Sexuality Education, 10, 333-350.
- Ginger, V. A. T., & Yang, C. C. (2011). Functional anatomy of the female sex organs. In Mulhall, J. P., Incrocci, L., Goldstein, I., & Rosen, R. (eds). Cancer and sexual health. Springer Publishing.
- Giorgi, G., & Siccardi, M. (1996). Ultrasonographic observation of a female fetus sexual behavior in utero [Letter to the editors]. American Journal of Obstetrics and Gynecology, 175,(3, Part 1).
- Google Search Statistics, http://www.internetlivestats.com/google-search-statistics/ Retrieved on May 5, 2017.
- Gott, M., & Hinchliff, S. (2003). Barriers to seeking treatment for sexual problems in primary care: A qualitative study with older people. Family Practice, 20, 690-695.
- Grumbach, M. M., & Conte, F. A. (1998). Disorders of sex differentiation. In: Wilson, J. D., Foster, D. W., Kronenborg, H. M., & Larsen, P. R. (Eds.) Williams Textbook of Endocrinology, Ed:9th. (pps. 1303-1425). Philadelphia: WB Saunders.
- Haffner, D. W. (1999). From diapers to dating: A parent\'s guide to raising sexually healthy children. New York, NY: Newmarket Press.
- Halata, Z., & Spaethe, A. (1997). Sensory innervation of the human penis. Advanced Experimental Medical Biology, 424, 265–266.
- Hall, S. A., Shackelton, R., Rosen, R. C., & Araujo, A. B. (2010). Sexual activity, erectile dysfunction, and incident cardiovascular events. American Journal of Cardiology, 105, 192-197.
- Herdt, G. (1996). Third sex, third gender–Beyond sexual dimorphism in culture and history. Cambridge: MIT Press.
- Hines, T. (2001). The G-Spot: A modern gynecologic myth. American Journal of Obstetrics and Gynecology, 185, 359–362.
- Igbinedion, B. O. E., & Akhigbe, T. O. (2012). The accuracy of 2D ultrasound prenatal sex determination. Nigerian Medical Journal: Journal of the Nigeria Medical Association, 53, 71–75.
- Jalili, C. (2016). Here’s what 2,000 men and women fear the most about sex. Elite Daily. http://elitedaily.com/dating/fears-sex-study/ Retrieved on May 10, 2017.
- Jannini, E. A., Rubio‐Casillas, A., Whipple, B., Buisson, O., Komisaruk, B. R., & Brody, S. (2012). Female orgasm(s): One, two, several. Journal of Sexual Medicine, 9, 956–965.
- Janssen, P. A., Thiessen, P., Klein, M. C., Whitfield, M. F., MacNab, Y. C., & Cullis-Kuhl, S. C. (2007). Standards for the measurement of birth weight, length and head circumference at term in neonates of European, Chinese and South Asian ancestry. Open Medicine, 1, e74–e88.
- Kilchevsky, A., Vardi, Y., Lowenstein, L., & Gruenwald, I. (2012). Is the female G-Spot truly a distinct anatomic entity? Sexual Medicine, 9, 719-726.
- Killick, S. R., Leary, C., Trussell, J., & Guthrie, K. A. (2011). Sperm content of pre-ejaculatory fluid. Human Fertility, 14, 48-52.
- King, B. M. (2015). Human Sexuality Today (7th ed.). Upper Saddle River, NJ: Prentice Hall.
- Kleinplatz, P. J. (2012). New directions in sex therapy: Innovations and alternatives. New York: Routledge.
- Komisaruk, B. R., Wise, N., Frangos, E., Liu, W., Allen, K., & Brody, S. (2011). Women\'s clitoris, vagina and cervix mapped on the sensory cortex: fMRI evidence. Journal of Sexual Medicine, 10, 822–830.
- Lucas, D. R., & Fox, J. (2018). The psychology of human sexuality. In R. Biswas-Diener & E. Diener (Eds), Noba textbook series: Psychology. Champaign, IL: DEF publishers. DOI:nobaproject.com).
- Lucas, D. R., Roberts, C., Nylander, G., & Higdon, M. (2016). Do Americans know more about sex today than they did 25 years ago? Paper presented at the annual meeting of the Southwestern Psychological Association, Dallas, Texas.
- Martinson, F. M. (1994). The sexual life of children. Westport, CT: Bergin & Garvey.
- Masters, W. H., & Johnson, V. E. (1966). Human Sexual Response. Boston: Little, Brown.
- McCabe, M.P., Sharlip, I.D., Lewis, R., Atalla, E., Balon, R., Fisher, A.D., Laumann, E., Lee, S.W., & Segraves, R.T. (2016). Incidence and prevalence of sexual dysfunction in women and men: A consensus statement from the fourth international consultation on sexual medicine 2015. The Journal of Sexual Medicine, 13, 144 -152.
- Molina G., Weiser, T.G., Lipsitz, S. R., Esquivel, M. M., Uribe-Leitz, T., Azad, T., Shah, N., Semrau, K., Berry, W. R., Gawande, A. A., & Haynes, A. B. Relationship between Cesarean delivery rate and maternal and neonatal mortality. Journal of the American Medical Association, 314, 2263-2270.
- Montague, D. K., Jarow, J. P., Broderick, G. A., et al. (2007). The management of erectile dysfunction: An update. The American Urological Association. Journal of Urology, June.
- Moore, K.T., Persaud, T.V.N., & Torchia, M.G. (2016). The developing human: Clinically oriented embryology. Philadelphia, PA: Elsevier, Inc.
- Munoz, K., Davtyan, M., & Brown, B. (2014). Revisiting the condom riddle: Solutions and implications. Electronic Journal of Human Sexuality, 17.
- Nappi, R. E., & Lachowsky, M. (2009). Menopause and sexuality: Prevalence of symptoms and impact on quality of life. Maturitas, 63, 138-141.
- Nguyen, N., & Holodniy, M. (2008). HIV infection in the elderly. Clinical Interventions in Aging, 3, 453–472.
- Nummenmaa, L., Suvilehto, J.T., Glerean, E., Santtila, P., & Hietanen, J. K. (2016). Topography of human erogenous zones. Archives of Sexual Behavior, 45, 1207-1216.
- Nuno, S. M. (2017). Let's talk about sex: The importance of open communication about sexuality before and during Relationships. In N. R. Stilton (Ed.), Family Dynamics and Romantic Relationships in a Changing Society (pp. 47-61). IGI Global.
- O'Connell, H.E., Sanjeevan, K.V., & Hutson, J. M. (2005). Anatomy of the clitoris. Journal of Urology, 174, 1189-1195.
- Odeh M., Ophir E., & Bornstein J. (2008). Hypospadias mimicking female genitalia on early second trimester sonographic examination. Journal of Clinical Ultrasound, 36, 581–583.
- Opperman, E., Braun, V., Clarke, V., & Rogers, C. (2014). It feels so good it almost hurts: Young adults experiences of orgasm and sexual pleasure. The Journal of Sex Research, 51, 503-515.
- Options for Sexual Health. Retrieved on July 2, 2017.
- Ortigue, S., Grafton, S. T., & Bianchi-Demicheli, F. (2007). Correlation between insula activation and self-reported quality of orgasm in women. Neuroimage, 37, 551-560.
- Owen, D. H., & Katz, D. F. (2005). A review of the physical and chemical properties of human semen and the formulation of a semen simulant. Journal of Andrology, 26, 459–469.
- Paik, A., Sanchagrin, K. J., & Heimer, K. (2016). Broken promises: Abstinence pledging and sexual and reproductive health. Journal of Marriage and Family, 78, 546-561.
- Parrot, A. (1994). Incest, infertility, infant sexuality. In Bullough, V. & Bullough, B. (Eds.), Human Sexuality Encyclopedia (pp. 289-310). New York, NY: Garland.
- Penfield, W., & Boldrey, E. (1937). Somatic motor and sensory representation in the cerebral cortex of man as studied by electrical stimulation. Brain, 60, 389-443.
- Porst, H., Montorsi, F., Rosen, R.C., Gaynor, L., Grupe, S., & Alexander, J. (2007). The Premature Ejaculation Prevalence and Attitudes (PEPA) survey: Prevalence, comorbidities, and professional help-seeking. European Urology, 51, 816–824.
- Rosen, R. C. (2000). Prevalence and risk factors of sexual dysfunction in men and women. Current Psychiatry Reports, 3,189-195.
- Rysavy, M. A., Li, L., Bell, E. F., Das, A., Hintz, S. R., Stoll, B. J., et al. (2015). Between-hospital variation in treatment and outcomes in extremely preterm infants. New England Journal of Medicine, 372, 1801–1811.
- Satterwhite, C. L., Torrone, E., Meites, E., Dunne, E. F., Mahajan, R., Ocfemia, M. C., Su, J., Xu, F., & Weinstock, H. (2013). Sexually transmitted infections among U.S. women and men: Prevalence and incidence estimates, 2008. Sexually Transmitted Diseases, 40, 187-193.
- Shah, J., & Christopher, N. (2002). Can shoe size predict penile length? British Journal of Urology International, 90, 586–587.
- Siminoski, K., & Bain, J. (1993). The relationships among height, penile length, and foot size. Annals of Sex Research, 6, 231-235.
- Simon, L., & Daneback, K. (2013). Adolescents’ use of the Internet for sex education: A thematic and critical review of the literature. International Journal of Sexual Health, 25, 305-319.
- Stephens-Davidowitz, S. (2015). Searching for sex. Sunday Review, New York Times, https://www.nytimes.com/2015/01/25/opinion/sunday/seth-stephens-davidowitz-searching-for-sex.html. Retrieved on May 5, 2017.
- Swaab, D. F. (2004). Sexual differentiation of the human brain: Relevance for gender identity, transsexualism and sexual orientation. Gynecological Endocrinology, 19, 301-312.
- Tachedjiana, G., Aldunatea, M., Bradshawe, C. S., & Coneg, R. A. (in press). The role of lactic acid production by probiotic Lactobacillus species in vaginal health. Research in Microbiology
- The Society of Obstetricians and Gynaecologists of Canada. Retrieved on July 2, 2017.
- Thompson, D. (2016). Anatomy may be key to female orgasm. https://consumer.healthday.com/sexual-health-information-32/orgasm-health-news-510/anatomy-may-be-key-to-female-orgasm-709934.html. Retrieved on March 25, 2017.
- Veale, D., Miles, S., Bramley, S., Muir, G. & Hodsoll, J. (2015). Am I normal? A systematic review and construction of nomograms for flaccid and erect penis length and circumference in up to 15,521 men. British Journal of Urology International, 115, 978–986.
- Weiss, R. (2014). Baby Boomers Gone Wild! Seniors and STDs. Psychology Today. https://www.psychologytoday.com/blog/love-and-sex-in-the-digital-age/201403/baby-boomers-gone-wild-seniors-and-stds Retrieved on May 6, 2017.
- Wessells, H., Lue, T.F., & McAninch, J. W. (1996). Penile length in the flaccid and erect states: Guidelines for penile augmentation. Journal of Urology, 156, 995-997.
- Wickman, D. (2017). Plasticity of the Skene\'s gland in women who report fluid ejaculation with orgasm. The Journal of Sexual Medicine, 14, S67.
- Wilcox, A. J., Dunson, D., & Baird, D. D. (2000). The timing of the “fertile window” in the menstrual cycle: Day specific estimates from a prospective study. British Medical Journal, 321, 1259-1262.
- Wisniewski, A. B., Migeon, C J., Meyer-Bahlburg, H. F., Gearhart, J. P., Berkovitz, G. D., Brown, T. R., & Money, J. (2000). Complete androgen insensitivity syndrome: Long-term medical, surgical, and psychosexual outcome. Journal of Clinical Endocrinology and Metabolism, 85, 2664–2669.
- Wizemann , T. M., & Pardue, M. L. (2001). Sex begins in the womb. In T. M. Wizemann & M. L. Pardue (Eds.), Exploring the Biological Contributions to Human Health: Does Sex Matter? Washington (DC): National Academies Press (US).
- World Health Organization (August 2016). Sexually transmitted infections (STIs). http://www.who.int/mediacentre/factsheets/fs110/en/ Retrieved May 6, 2017.
Authors
 Don LucasDr. Don Lucas is a Professor of Psychology and Coordinator of the Psychology Department at Northwest Vista College in San Antonio, Texas. His teaching over the past three decades has earned him a number of accolades, including the Minnie Stevens Piper Professor Award. He is the author of Being: Your Happiness, Pleasure, and Contentment.
Don LucasDr. Don Lucas is a Professor of Psychology and Coordinator of the Psychology Department at Northwest Vista College in San Antonio, Texas. His teaching over the past three decades has earned him a number of accolades, including the Minnie Stevens Piper Professor Award. He is the author of Being: Your Happiness, Pleasure, and Contentment. Jennifer FoxJennifer Fox is an Assistant Professor of Psychology and Advisor of Psi Beta at Northwest Vista College in San Antonio, Texas. As a Human Sexuality Educator and a mother of a spirited 6-year-old daughter, she is passionate about promoting sexual literacy for all ages.
Jennifer FoxJennifer Fox is an Assistant Professor of Psychology and Advisor of Psi Beta at Northwest Vista College in San Antonio, Texas. As a Human Sexuality Educator and a mother of a spirited 6-year-old daughter, she is passionate about promoting sexual literacy for all ages.
Creative Commons License



 Human Sexual Anatomy and Physiology by Don Lucas and Jennifer Fox is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Permissions beyond the scope of this license may be available in our Licensing Agreement.
Human Sexual Anatomy and Physiology by Don Lucas and Jennifer Fox is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Permissions beyond the scope of this license may be available in our Licensing Agreement.